(Originally posted on the National Physicians Alliance blog November 4, 2012)
--------------------
Physicians must care about our patients. In every decision we make
and each action we take, the health and wellness of our patients and our
communities must be at the center of what we do. The Affordable Care
Act (ACA) will make your healthcare better.
Our organization--the National Physicians Alliance (NPA)--was formed
in 2005 and is committed to advancing the core values of the medical
profession: service, integrity, and advocacy. The organization has key guiding principles that
focus on putting our patients health and wellness above all other
concerns. NPA's advocacy has emphasized the need to ensure patient
protection and to repair the broken covenant that
our nation's healthcare system must benefit all Americans. Our
commitment and our obligation to care for our patients is limited by
many factors: insurance company policies that restrict the care we can
provide, health disparities that persist despite individual efforts to
address them, and a lack of insurance that limits access to health
insurance and healthcare.
As a result of NPA's determination to ensure equitable and affordable healthcare for all Americans,
the organization has worked to secure the passage of the ACA and to
advocate for its full implementation. In keeping with NPA's guiding
principles, our support of the ACA has been focused on the benefits the
law provides to patients as well as its protection of the doctor-patient
relationship we hold as a sacred responsibility as professionals.
How does the ACA protect patients?
The ACA provides important benefits for ALL Americans: The ACA provides multiple benefits for the middle class. Considering the major role that healthcare costs play in personal bankruptcies
(PDF), it is clear that ensuring the affordability of healthcare
provides a crucial protection for middle class Americans. Affordable
insurance--made more so by government support to help lower income
families and changes in insurance enrollment that are predicted to
reduce the cost for all--will allow most Americans to see the health benefits of having health insurance
(PDF). Adult children will now be able to stay on parents' insurance
policies until they are 26 years old, thereby enhancing their ability to
access health insurance
while in school and starting out in the workforce. Coupled with
reforms that will remove limits on annual and lifetime coverage benefits
for patients, Americans will be better protected as they look to move
into the middle class and secure a better future for themselves and
their families. In addition, preventive care services including
vaccines, pap smears, colonoscopies, and other necessary services will
be made available to Americans without requiring co-pays, making them
more available than ever before.
The ACA promotes fairness and equality in medical care: The ACA reverses one of the most egregious facts of healthcare insurance in the US: the fact that a person's gender was the basis for charging women more for health insurance than men. This difference exists only because a woman was a woman, and is not due to specific coverage (PDF) such as for pregnancy or maternity care. The ACA will also target national healthcare inequalities
by strengthening the nation's community health centers, increasing the
number of physicians working in medically underserved areas by increasing National Health Service Corps scholarships. Finally, the ACA begins to address our national need for more primary care physicians and move towards a healthcare workforce that is accessible to all.
The ACA protects patients from insurance company abuses:
Thanks to the ACA, insurance companies will have less control over
patients' healthcare. Insurers will be required to offer insurance to
everyone regardless of whether or not they have a preexisting medical
condition--a benefit that has already gone into effect for children
and is planned to go into effect for adults in 2014. The ACA prevents
insurance companies from setting arbitrary limits to patients' lifetime
health insurance benefits, and as of 2014 will eliminate annual limits
to care. Insurance companies are required to spend 80-85% of members' premiums on providing benefits to those members,
as opposed to using that money for administrative costs or executive
salaries. The ACA bans the practice of rescissions, in which insurance
companies would seek reasons to retroactively cancel members' insurance
coverage once those members became ill and most needed the protection.
The ACA provides greater governmental scrutiny of unreasonable insurance rate hikes,
helping insure that Americans are not being harmed by insurers
willfully increasing policy costs without reason or justification.
Finally, by establishing health insurance marketplaces (or exchanges),
the ACA will require all insurers to show the purchasers of their
products--our patients--that the companies are effective and responsive
to their customers' needs or they will risk patients finding coverage
elsewhere. This should increase transparency and provide greater
benefits to patients who will be able to vote with their feet and leave
ineffective companies to look for better options.
The NPA is not the only physician organization to support the ACA. The law is also supported by the American Medical Association, the American Academy of Pediatrics, the American Academy of Family Physicians, the American College of Physicians, the American Congress of Obstetricians and Gynecologists, the Association of American Medical Colleges, and the American Osteopathic Association.
The reasons all of these physician groups support the ACA is simple.
As physicians, the law's reforms allow us to provide better care for
our patients--without being limited by insurance regulations or lack of
access to health insurance. The ACA removes important barriers to care,
and lets us get back to the core focus of our profession: the covenant
to do whatever we can to improve our patients' health and wellness.
Sunday, November 4, 2012
Sunday, October 28, 2012
Partnering with communities: why and how?
To enhance the impact medicine can have in addressing healthcare disparities, it is often necessary to work outside of the clinical space. One-on-one clinical care is critically important for the individual, but can only address the individual's need at that point in time. Although this is the core of medicine--the doctor/patient relationship--it is not sufficient to address broader issues.
I believe that physicians' roles in leadership and community focus require us to look beyond the clinic to bring necessary change. At the minimum, I believe that physicians need to be advocates for necessary change: at the organizational and/or at the political level, we must be pushing for policies that will improve the health of our communities.
At the same time, it can often very valuable to develop partnerships in the community itself. However one defines community, the community's members will have a strong sense of the community's strengths, needs, and challenges. However, in many cases forming a productive and effective relationship with underserved communities can be challenging. Many times, these communities may feel isolated and marginalized. In some cases, they may actively distrust medical institutions based on past experiences.
Every community is unique, and effective community partnerships will all differ in some way. However, there are some general themes that can guide the process in developing community partnerships:
I believe that physicians' roles in leadership and community focus require us to look beyond the clinic to bring necessary change. At the minimum, I believe that physicians need to be advocates for necessary change: at the organizational and/or at the political level, we must be pushing for policies that will improve the health of our communities.
At the same time, it can often very valuable to develop partnerships in the community itself. However one defines community, the community's members will have a strong sense of the community's strengths, needs, and challenges. However, in many cases forming a productive and effective relationship with underserved communities can be challenging. Many times, these communities may feel isolated and marginalized. In some cases, they may actively distrust medical institutions based on past experiences.
Every community is unique, and effective community partnerships will all differ in some way. However, there are some general themes that can guide the process in developing community partnerships:
- Demonstrate genuine commitment
- Have a long time horizon--things will move slower than you would prefer
- Assess the communities needs and values, and respect them
- Expect challenges and strife: pre-empt them if you can, address them when needed
- Understand that all decisions carry political consequences
- Good intentions are dangerous things: consider the ethics of your intervention
Identify and engage the community's leadership (official and unofficial) - Inspiration and interest on our part can help generate an idea, but need community guidance for any intervention
- Listen, think, talk...then act
- Tolerate of uncertainty
- Know that communities are heterogeneous, even if there are not any apparent differences on the surface
- Align incentives: look for space where your interests/motivations/rewards align with the community's
Wednesday, July 18, 2012
If it is a problem, why don't you have a solution?
First published on the OccupyHealthcare blog, July 18 2012.
--------------------
Just about three weeks ago, the Supreme Court ruled that the Patient Protection and Affordable Care Act (ACA) was constitutional in its requirement that all Americans have health insurance. However, the court also decided that the ACA's expansion of Medicaid eligibility and coverage could not be forced upon the states. States could opt to expand Medicaid as the law required, but those states that choose not to expand would not face the loss of their current Medicaid funding. Already, a number of Governors have declared their opposition to this Medicaid expansion.
The ACA's expansion of Medicaid is an important part of the law's efforts to expand coverage and healthcare access to most Americans. The law would require the expansion of Medicaid to cover individuals up to 133% of the Federal poverty level. The Federal government will pay 100% of this expansion for the first three years, a level of support that gradually lowers to 90% over the next five years. It is expected that, as designed, the ACA's Medicaid expansion would provide coverage to 17 million Americans. The law's new health insurance exchanges, that facilitate individuals' purchase of health insurance and provides subsidies for those with incomes between 133% and 400% Federal poverty level, would account for the rest of the ACA's increase in health insurance coverage.
Late last week, the Republican Governors Association (RGA) sent the Obama Administration a letter outlining their concerns about the proposed Medicaid expansion and the ACA's health insurance exchanges. The letter, signed by Virginia Governor Bob McDonnell, has one particularly notable passage:

The reason this passage struck me is because of its chutzpah. The RGA's own members are those who will make the decisions for their states as to whether or not the state will expand Medicaid coverage. However, if the state chooses not to, it is somehow the fault of the Administration for not having come up with an alternative plan. The letter purports to show concern for those low-income Americans who would have been covered by the Medicaid expansion (if not for the Governors' decisions to reject it), and expects the federal government to provide a means of coverage for these low-income individuals.
Of course, the ACA does provide a means for low-income people to access health insurance: it expands Medicaid. The RGA's letter is absurd, essentially saying: "If we reject the remedy you have developed to cover low-income Americans, you must come up with an alternative." This is even more striking if one reviews the underlying reasons why the states might reject the Medicaid expansion: they claim it is a violation of states' rights. If the states are worried about expansion of federal power, how is asking the Federal government for an answer to a state's own rate of uninsured individuals in any way logical? If anything, the states should be fixing this problem themselves if they were following their argument to its logical conclusion. Instead of asking for Federal help, the states should have already addressed this issue.
The states that have already rejected the ACA's Medicaid expansion include Texas and Florida. Both states are among those with the highest rates of uninsured.

Mississippi is second on this list, and is also considering rejecting the Medicaid expansion. The states whose residents would gain the most in terms of access to health insurance are those who are fighting this increase in access. These three states also have Republican governors, who have not come up with a better plan to improve access to insurance as of yet. If Republican governors truly thought that low-income Americans' access to health insurance was a problem, they have had ample time to come up with a solution...and they have not done so.
Medicaid coverage improves health outcomes, with the trade-off of an initial cost increase (possibly as those who have been insured finally access care). With the Federal government covering 100% of the initial expansion, they (not the states) would be paying for these up-front costs. Given that Medicaid is more cost-effective than private insurers (point 7 on this list), expanding access to health insurance via a program that is both cost-effective and beneficial is a smart move. Meanwhile, we know that being uninsured is bad for one's health.
Thanks to the ACA, we now have the tools to expand health insurance--and health care--to 30 million more Americans. Those who decry the law's reforms have, for the most part, failed to act in their own states and have failed to present a viable alternative. If the ACA's opponents thought the issues of heath insurance and access to health care were a problem, they would have acted long ago. It is time for them to stop obstructing this important step forward to improve Americans' health.
--------------------
Just about three weeks ago, the Supreme Court ruled that the Patient Protection and Affordable Care Act (ACA) was constitutional in its requirement that all Americans have health insurance. However, the court also decided that the ACA's expansion of Medicaid eligibility and coverage could not be forced upon the states. States could opt to expand Medicaid as the law required, but those states that choose not to expand would not face the loss of their current Medicaid funding. Already, a number of Governors have declared their opposition to this Medicaid expansion.
The ACA's expansion of Medicaid is an important part of the law's efforts to expand coverage and healthcare access to most Americans. The law would require the expansion of Medicaid to cover individuals up to 133% of the Federal poverty level. The Federal government will pay 100% of this expansion for the first three years, a level of support that gradually lowers to 90% over the next five years. It is expected that, as designed, the ACA's Medicaid expansion would provide coverage to 17 million Americans. The law's new health insurance exchanges, that facilitate individuals' purchase of health insurance and provides subsidies for those with incomes between 133% and 400% Federal poverty level, would account for the rest of the ACA's increase in health insurance coverage.
Late last week, the Republican Governors Association (RGA) sent the Obama Administration a letter outlining their concerns about the proposed Medicaid expansion and the ACA's health insurance exchanges. The letter, signed by Virginia Governor Bob McDonnell, has one particularly notable passage:
The reason this passage struck me is because of its chutzpah. The RGA's own members are those who will make the decisions for their states as to whether or not the state will expand Medicaid coverage. However, if the state chooses not to, it is somehow the fault of the Administration for not having come up with an alternative plan. The letter purports to show concern for those low-income Americans who would have been covered by the Medicaid expansion (if not for the Governors' decisions to reject it), and expects the federal government to provide a means of coverage for these low-income individuals.
Of course, the ACA does provide a means for low-income people to access health insurance: it expands Medicaid. The RGA's letter is absurd, essentially saying: "If we reject the remedy you have developed to cover low-income Americans, you must come up with an alternative." This is even more striking if one reviews the underlying reasons why the states might reject the Medicaid expansion: they claim it is a violation of states' rights. If the states are worried about expansion of federal power, how is asking the Federal government for an answer to a state's own rate of uninsured individuals in any way logical? If anything, the states should be fixing this problem themselves if they were following their argument to its logical conclusion. Instead of asking for Federal help, the states should have already addressed this issue.
The states that have already rejected the ACA's Medicaid expansion include Texas and Florida. Both states are among those with the highest rates of uninsured.

Mississippi is second on this list, and is also considering rejecting the Medicaid expansion. The states whose residents would gain the most in terms of access to health insurance are those who are fighting this increase in access. These three states also have Republican governors, who have not come up with a better plan to improve access to insurance as of yet. If Republican governors truly thought that low-income Americans' access to health insurance was a problem, they have had ample time to come up with a solution...and they have not done so.
Medicaid coverage improves health outcomes, with the trade-off of an initial cost increase (possibly as those who have been insured finally access care). With the Federal government covering 100% of the initial expansion, they (not the states) would be paying for these up-front costs. Given that Medicaid is more cost-effective than private insurers (point 7 on this list), expanding access to health insurance via a program that is both cost-effective and beneficial is a smart move. Meanwhile, we know that being uninsured is bad for one's health.
Thanks to the ACA, we now have the tools to expand health insurance--and health care--to 30 million more Americans. Those who decry the law's reforms have, for the most part, failed to act in their own states and have failed to present a viable alternative. If the ACA's opponents thought the issues of heath insurance and access to health care were a problem, they would have acted long ago. It is time for them to stop obstructing this important step forward to improve Americans' health.
Friday, June 29, 2012
The healthcare aftermath of June 28, 2012: What we protected, what is missing, and what we still need to do
(Originally posted on the OccupyHealthcare blog June 28, 2012)
--------------------
Yesterday, the Supreme Court upheld the constitutionality of the Patient Protection and Affordable Care Act (PPACA). After nearly 2 1/2 years of partisan misinformation, the Court has established the law's legitimacy.
This is an enormous step forward. The PPACA incorporates many patient protections that will reduce the profit-centered influence of for-profit insurance companies on American's healthcare. Once the law is fully implemented in 2014, insurers will no longer be able to deny insurance coverage to any American even if they have pre-exisiting medical illnesses and will no longer be able to place yearly or lifetime limits on members' benefits. Insurance companies will be required to spend 80-85% of the money members pay in premiums on providing benefits to members as opposed to salaries and administrative costs. Young adults will be able to stay on parents' insurance plans until they turn 26--meaning that they can keep necessary insurance coverage as they finish their educations or start their careers. Federal subsidies will make insurance affordable for Americans who are not offered insurance through their jobs and cannot afford to purchase it on their own. Private insurers have called the shots for too long, and restricted access to necessary care for Americans who could not afford it or who were already ill. These days are now coming to an end.
The PPACA also addresses key needs in our healthcare system. It will strengthen our primary care workforce and our community health centers. It will encourage research that is both patient-centered and evidence-based, to help patients and physicians make informed decisions about the best approaches to individuals' care. The PPACA also makes preventive care available for all without co-pays, allowing healthcare providers to detect and treat (or even prevent) chronic disease before they cause permanent harm. The law will increase Medicaid access and will strengthen Medicare. Finally, the PPACA includes programs to explore new ways of providing (and paying for) healthcare services that are more effective, more coordinated, and less expensive.
All of these are critical patient protections and healthcare system reforms. The protections will allow us to make sure that healthcare is available with less interference on the part of insurance companies and reforms the most egregious insurance company practices. The reforms will allow us to start to move our healthcare system away from one providers are paid more for doing more care and towards a system that provides better care. These are significant steps, and reforms that the Supreme Court has now endorsed and guaranteed so long as the Affordable Care Act is in effect.
However, the law is an incomplete step forward. It still leaves a number of Americans lacking health insurance, and explicitly prevents many immigrants from accessing care. The PPACA supports private, for-profit insurance companies with public money in the form of subsidies to help low-income Americans pay for insurance. There were still be fragmented care as patients will still move between private and public insurances or between private insurers. There is little in the law to address the high and increasing costs of pharmaceuticals and medical devices. By building upon the flawed structure of individual private insurance companies, the PPACA cannot offer the savings inherent in single-payer systems where administrative costs are lowered, coverage and access are assured to all. The political environment in Washington, DC would not allow for such a significant move as a single-payer system. In fact, the law barely survived in its current form. This does not mean that we should rest on our laurels: even with the PPACA's reforms there will be much more work to do.
We must monitor how the PPACA is enacted, and we must avoid its reforms being co-opted or weakened by special interests and the law's stubborn opponents. Where the law does not meet its intended results, we must revise it to ensure that it will. We must identify those who do not benefit from the law as written and work to find ways to extend the law's benefits to all. We must continue to speak about the law's benefits and make sure that our friends, families, and colleagues understand how very important this law is.
We must be vigilant heading forward. Although the PPACA is constitutional, congressional opponents can continue their attempts to repeal and defund the law. Rest assured that, if they are able to, they will do just that. The House is already planning a repeal vote on July 11. Under the PPACA, the economic and human costs of allowing millions of Americans to go without health care are finally being addressed. We cannot afford to take any steps backwards: there is still a long road ahead.
--------------------
Yesterday, the Supreme Court upheld the constitutionality of the Patient Protection and Affordable Care Act (PPACA). After nearly 2 1/2 years of partisan misinformation, the Court has established the law's legitimacy.
This is an enormous step forward. The PPACA incorporates many patient protections that will reduce the profit-centered influence of for-profit insurance companies on American's healthcare. Once the law is fully implemented in 2014, insurers will no longer be able to deny insurance coverage to any American even if they have pre-exisiting medical illnesses and will no longer be able to place yearly or lifetime limits on members' benefits. Insurance companies will be required to spend 80-85% of the money members pay in premiums on providing benefits to members as opposed to salaries and administrative costs. Young adults will be able to stay on parents' insurance plans until they turn 26--meaning that they can keep necessary insurance coverage as they finish their educations or start their careers. Federal subsidies will make insurance affordable for Americans who are not offered insurance through their jobs and cannot afford to purchase it on their own. Private insurers have called the shots for too long, and restricted access to necessary care for Americans who could not afford it or who were already ill. These days are now coming to an end.
The PPACA also addresses key needs in our healthcare system. It will strengthen our primary care workforce and our community health centers. It will encourage research that is both patient-centered and evidence-based, to help patients and physicians make informed decisions about the best approaches to individuals' care. The PPACA also makes preventive care available for all without co-pays, allowing healthcare providers to detect and treat (or even prevent) chronic disease before they cause permanent harm. The law will increase Medicaid access and will strengthen Medicare. Finally, the PPACA includes programs to explore new ways of providing (and paying for) healthcare services that are more effective, more coordinated, and less expensive.
All of these are critical patient protections and healthcare system reforms. The protections will allow us to make sure that healthcare is available with less interference on the part of insurance companies and reforms the most egregious insurance company practices. The reforms will allow us to start to move our healthcare system away from one providers are paid more for doing more care and towards a system that provides better care. These are significant steps, and reforms that the Supreme Court has now endorsed and guaranteed so long as the Affordable Care Act is in effect.
However, the law is an incomplete step forward. It still leaves a number of Americans lacking health insurance, and explicitly prevents many immigrants from accessing care. The PPACA supports private, for-profit insurance companies with public money in the form of subsidies to help low-income Americans pay for insurance. There were still be fragmented care as patients will still move between private and public insurances or between private insurers. There is little in the law to address the high and increasing costs of pharmaceuticals and medical devices. By building upon the flawed structure of individual private insurance companies, the PPACA cannot offer the savings inherent in single-payer systems where administrative costs are lowered, coverage and access are assured to all. The political environment in Washington, DC would not allow for such a significant move as a single-payer system. In fact, the law barely survived in its current form. This does not mean that we should rest on our laurels: even with the PPACA's reforms there will be much more work to do.
We must monitor how the PPACA is enacted, and we must avoid its reforms being co-opted or weakened by special interests and the law's stubborn opponents. Where the law does not meet its intended results, we must revise it to ensure that it will. We must identify those who do not benefit from the law as written and work to find ways to extend the law's benefits to all. We must continue to speak about the law's benefits and make sure that our friends, families, and colleagues understand how very important this law is.
We must be vigilant heading forward. Although the PPACA is constitutional, congressional opponents can continue their attempts to repeal and defund the law. Rest assured that, if they are able to, they will do just that. The House is already planning a repeal vote on July 11. Under the PPACA, the economic and human costs of allowing millions of Americans to go without health care are finally being addressed. We cannot afford to take any steps backwards: there is still a long road ahead.
Monday, June 25, 2012
Global Health and Underserved Communities: Challenges and Rewards
From May 29 to June 9, I traveled on a medical relief trip to the Dominican Republic. Below is the text of an e-mail I sent the team, which I include here because I believe it states my position on the challenges and rewards that one can attain for working with underserved communities in the US and overseas.
--------------------
I wanted to send this note to thank everyone for their hard work and for making the trip successful. For those new to global health projects such as this, I realize it is a difficult adjustment to make: the long hours, the constant work, the uncertainty around schedules and plans, and the constant feel that we should, somehow, be doing more than we are. The recognition that the need is greater than our ability to respond to it, and how we can come to terms with that without necessarily accepting it, and how we can use our resources and skills to do our part in helping the patients we work with.
--------------------
I wanted to send this note to thank everyone for their hard work and for making the trip successful. For those new to global health projects such as this, I realize it is a difficult adjustment to make: the long hours, the constant work, the uncertainty around schedules and plans, and the constant feel that we should, somehow, be doing more than we are. The recognition that the need is greater than our ability to respond to it, and how we can come to terms with that without necessarily accepting it, and how we can use our resources and skills to do our part in helping the patients we work with.
This
is a heavy task: in healthcare, we all would like to think that we can
make big differences through our profession, when the humbling truth is
that often the best we can do is to be a small part of a larger
process. I believe we are obligated to help our patients to the extend
of their needs and to the best of our abilities, but this means that
there will always be someone who we could not reach, or for whom our
skills were not sufficient.
This
is not a comfortable place to be, whether in the US or overseas. I
think working in developing nations makes this gap between resources and
needs more evident, but as you continue your training in Richmond you
will start to notice more and more examples of the mismatch between what
people need and what we can offer.
The
best approach to help as many people as possible is to determine where
you can have an impact, and to work as a team to get the most out of
what we have. We chose to put a lot of focus on diabetes and high blood
pressure because, as medical and pharmacy professionals, this is where
our greatest skill set lies. However, our summer clinical work fits
into the larger picture of our ongoing community development work in the
Dominican Republic: work that aims to address sanitation, flooding, and
other broad social determinants of health. The fact that our ongoing
commitment to the community leverages our skills and matches them to
with community development project allows us to address health on many
more levels than if these two initiatives were separate. We may have
only done a small part, but it is a small part of a greater whole.
At
the same time, our part was not especially small. In the community, we
provided healthcare to nearly 500 people: people who would have lacked
care if we were not present. For some, this involved treating blood
pressure and other chronic illness. For some, this involved parasite
medications and vitamins to enhance nutrition. For some this involved
coming to get medications to use if problems such as back pain or
stomach pain developed in the future. However, I was taught that the role of a healer is to "cure
sometimes, relieve often, comfort always" and, as with that as a
guiding principle, I believe that there is value in doing our best to
care for everyone regardless of the objective severity of their illness.
It would have been impossible to
have seen the over 600 patients (when both clinical sites are added up)
without teamwork, collaboration, and a unified sense of mission.
Despite the challenges noted above, you responded brilliantly. Whether
working registration, vitals, pharmacy or seeing patient, everyone
willingly stepped forward to do what needed to be done to make sure that
we met our commitments to our patients and to each other.
For all of this, I thank each and
every one of you for being part of this exceptional team. I look
forward to working with some (many? all?) of you again in the future.
Sunday, June 24, 2012
#MedRead (part 3): Non-fiction books: Health policy, healthcare reform, and healthcare redesign
Recently, I made a request on Twitter for suggestions for books that
medical students should read. These suggestions could be books of any
sort: fiction, non-fiction, clinically-focused, etc. I was hoping to
get suggestions for books that made a meaningful impact on people. I'll
be posting the lists in a series of blog posts.
In each case, I've linked the book title to its Powells.com listing...mainly because I didn't want to link to larger sites such as Amazon. In practice, I would strongly advise looking for these books at the library (to test them out--use this site to find the books at a library near you) or at your local independent bookstore (such as Chop Suey Books, in Richmond). Remember that if you're local bookseller doesn't carry these titles, they can probably order them for you--and they'll keep your money local.
Alternately, if you wish to support the authors directly, feel free to see if you can purchase the book you are interested in from the author's own website.
This is the third installment, focused on health policy, healthcare reform, and healthcare redesign. The first installment is here, and the second is here.
Pathologies of Power – Paul Farmer
Landmark: The Inside Story of America's New Health Care Law, and What It Means For Us All – Washington Post Staff
Understanding Health Policy -- Bodenheimer and Grumbach
The Social Transformation of American Medicine – Paul Starr
The Last Well Person: How To Stay Well Despite The Health-Care System – Nortin Hadler
The Truth About the Drug Companies: How They Deceive Us and What to Do about It – Marcia Angell
Selling Sickness: How the World's Biggest Pharmaceutical Companies Are Turning Us All Into Patients – Ray Moynihan
Overtreated: Why Too Much Medicine Is Making Us Sicker and Poorer – Shannon Brownlee
Overdosed America: The Broken Promise of American Medicine – John Abramson
Creative Destruction of Medicine: How the Digital Revolution will Create Better Healthcare – Eric Topol
Time To Die : How American Hospitals Shape the End of Life – Sharon Kaufman
Let the Record Show: Medical Malpractice, the Lawsuit Nobody Wins – J. Kelley Avery
AMA Code of Medical Ethics
Money Driven Medicine: The Real Reason Healthcare Costs so Much – Maggie Mahar
Health Care Will Not Reform Itself: A User's Guide to Refocusing and Reforming American Health Care – George C. Halvorson
Through the Patients’ Eyes: Understanding and Promoting Patient-Centered Care – Margaret Gerteis
Caring for the Country: Family Doctors in Small Rural Towns – Howard Rabinowitz
Beliefs and Families: A Model for Healing Illness – Lorraine M. Wright, Wendy Watson, and Janice M. Bell
On the Take: How Medicine's Complicity with Big Business Can Endanger Your Health – Jerome P. Kassirer
The Patient Paradox: Why Sexed Up Medicine Is Bad for Your Health – Margaret Mccartney (A more-detailed description can be found here.)
If you have read these books (or if you recommended them), please use the comments below to provide us with some thoughts on why the book mattered to you.
In each case, I've linked the book title to its Powells.com listing...mainly because I didn't want to link to larger sites such as Amazon. In practice, I would strongly advise looking for these books at the library (to test them out--use this site to find the books at a library near you) or at your local independent bookstore (such as Chop Suey Books, in Richmond). Remember that if you're local bookseller doesn't carry these titles, they can probably order them for you--and they'll keep your money local.
Alternately, if you wish to support the authors directly, feel free to see if you can purchase the book you are interested in from the author's own website.
This is the third installment, focused on health policy, healthcare reform, and healthcare redesign. The first installment is here, and the second is here.
Pathologies of Power – Paul Farmer
Landmark: The Inside Story of America's New Health Care Law, and What It Means For Us All – Washington Post Staff
Understanding Health Policy -- Bodenheimer and Grumbach
The Social Transformation of American Medicine – Paul Starr
The Last Well Person: How To Stay Well Despite The Health-Care System – Nortin Hadler
The Truth About the Drug Companies: How They Deceive Us and What to Do about It – Marcia Angell
Selling Sickness: How the World's Biggest Pharmaceutical Companies Are Turning Us All Into Patients – Ray Moynihan
Overtreated: Why Too Much Medicine Is Making Us Sicker and Poorer – Shannon Brownlee
Overdosed America: The Broken Promise of American Medicine – John Abramson
Creative Destruction of Medicine: How the Digital Revolution will Create Better Healthcare – Eric Topol
Time To Die : How American Hospitals Shape the End of Life – Sharon Kaufman
Let the Record Show: Medical Malpractice, the Lawsuit Nobody Wins – J. Kelley Avery
AMA Code of Medical Ethics
Money Driven Medicine: The Real Reason Healthcare Costs so Much – Maggie Mahar
Health Care Will Not Reform Itself: A User's Guide to Refocusing and Reforming American Health Care – George C. Halvorson
Through the Patients’ Eyes: Understanding and Promoting Patient-Centered Care – Margaret Gerteis
Caring for the Country: Family Doctors in Small Rural Towns – Howard Rabinowitz
Beliefs and Families: A Model for Healing Illness – Lorraine M. Wright, Wendy Watson, and Janice M. Bell
On the Take: How Medicine's Complicity with Big Business Can Endanger Your Health – Jerome P. Kassirer
The Patient Paradox: Why Sexed Up Medicine Is Bad for Your Health – Margaret Mccartney (A more-detailed description can be found here.)
If you have read these books (or if you recommended them), please use the comments below to provide us with some thoughts on why the book mattered to you.
Tuesday, June 12, 2012
ACA triggers insurer reforms...but the law is still necessary.
(First published on the National Physicians Alliance blog, June 12 2012)
--------------------
Yesterday, three major insurers announced that they would keep in place major insurance reforms introduced in the Patient Protection and Affordable Care Act (ACA), regardless of how the Supreme Court decides regarding the law's constitutionality.
UnitedHealth, Aetna, and Humana all announced that they would continue allowing children under age 26 to remain on parents' health insurance plans, allow independent appeals of insurance decisions, and cover certain preventive services.
Although this move by these for-profit insurers appears to be a good thing, there are two important considerations to remember. The first is that none of these insurers have agreed to issue insurance plans regardless of pre-existing conditions. If an individual with prior medical problems applies for insurance from these organizations, the insurers can still deny coverage. This would no longer be possible once the ACA is fully implemented. Therefore, the law is still critically important to make sure that all Americans will have access to health insurance coverage.
The second consideration is that the ACA was the catalyst for insurers to change their practices. For-profit insurers have been around for a long time, and had plenty of opportunity to implement these reforms on their own. However, none did until the ACA was passed and signed into law. The provisions that the insurers plan to keep in place are the law's most popular provisions, but they were not established by the insurers in a vacuum. The ACA put these reforms in place, the public realized that they were beneficial, and now the insurers have decided to reform their practices accordingly. If not for the ACA, I deeply doubt we would have seen any sort of insurance reforms of this sort. In fact, when the law was being developed, insurers defended their rights to rescind patients' coverage. The ACA deserves full credit for forcing insurers to enact these important patient protection reforms.
Despite the fact that insurers have belatedly agreed to support these patient protections, the law is still critically important:
The ACA has forced insurers to make some meaningful changes in how they practice--changes the insurers had given no indication they would enact on their own. This shows the law's power and effectiveness: thanks to the ACA, millions of Americans will have more robust insurance coverage, regardless of the Supreme Court's decision. However, what the private insurers have omitted from their promises to extend the ACA's benefits shows why we still need this important piece of healthcare reform: it is a critical step to ensure affordable and accessible healthcare insurance for all.
--------------------
Yesterday, three major insurers announced that they would keep in place major insurance reforms introduced in the Patient Protection and Affordable Care Act (ACA), regardless of how the Supreme Court decides regarding the law's constitutionality.
UnitedHealth, Aetna, and Humana all announced that they would continue allowing children under age 26 to remain on parents' health insurance plans, allow independent appeals of insurance decisions, and cover certain preventive services.
Although this move by these for-profit insurers appears to be a good thing, there are two important considerations to remember. The first is that none of these insurers have agreed to issue insurance plans regardless of pre-existing conditions. If an individual with prior medical problems applies for insurance from these organizations, the insurers can still deny coverage. This would no longer be possible once the ACA is fully implemented. Therefore, the law is still critically important to make sure that all Americans will have access to health insurance coverage.
The second consideration is that the ACA was the catalyst for insurers to change their practices. For-profit insurers have been around for a long time, and had plenty of opportunity to implement these reforms on their own. However, none did until the ACA was passed and signed into law. The provisions that the insurers plan to keep in place are the law's most popular provisions, but they were not established by the insurers in a vacuum. The ACA put these reforms in place, the public realized that they were beneficial, and now the insurers have decided to reform their practices accordingly. If not for the ACA, I deeply doubt we would have seen any sort of insurance reforms of this sort. In fact, when the law was being developed, insurers defended their rights to rescind patients' coverage. The ACA deserves full credit for forcing insurers to enact these important patient protection reforms.
Despite the fact that insurers have belatedly agreed to support these patient protections, the law is still critically important:
- Not all insurers have agreed to sustain these important reforms. Blue Cross/Blue Shield, Wellpoint, and Cigna are hedging their bets until the Supreme Court's decision is known and declined to make any commitments in response to yesterday's announcements from UnitedHealth, Aetna and Humana. Considering the size of these insurers, this would place many Americans at risk of losing insurance coverage if the ACA's protections were lost.
- The ACA provides subsidies for Americans who cannot afford to pay for private insurance out-of-pocket. These subsidies make health insurance, which is otherwise prohibitively expensive for many Americans, affordable and available. Without the ACA, the insurers could claim to make their coverage available to many in the sense that it is technically available, but could price it at a level that places it out of reach.
- One of the major ways that the ACA will expand insurance coverage is by expanding Medicaid. This will provide access to health insurance for millions of low-income Americans, something that these actions by the insurance companies will not affect.
- The ACA requires private insurers to spend 80-85% of the money they receive in premium payments on providing health care services (instead of using this money for administrative costs, salaries, etc). This is known as the medical loss ratio (MLR). The ACA's MLR requirements will mean that the money individuals pay to ensure they have insurance coverage will actually be used to provide insurance benefits. None of the insurance companies have pledged to maintain this ratio heading forward should the ACA be overturned.
The ACA has forced insurers to make some meaningful changes in how they practice--changes the insurers had given no indication they would enact on their own. This shows the law's power and effectiveness: thanks to the ACA, millions of Americans will have more robust insurance coverage, regardless of the Supreme Court's decision. However, what the private insurers have omitted from their promises to extend the ACA's benefits shows why we still need this important piece of healthcare reform: it is a critical step to ensure affordable and accessible healthcare insurance for all.
Sunday, April 29, 2012
The Cost Depends on the Value
(Initially published April 27, 2012 on the OccupyHealthcare blog.)
--------------------
Last week, Medscape released the results of their 2011 survey of physician compensation:
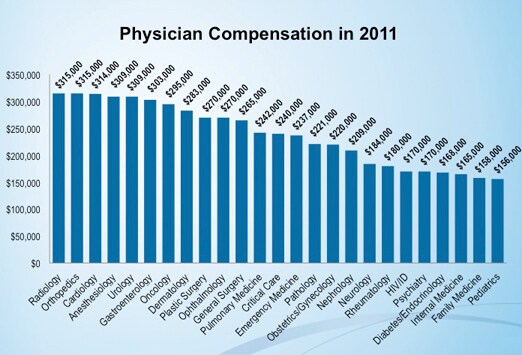
I share this post here to point out the discrepancy in physicians' average salaries based on their specialties. In particular, I would like to highlight that the three lowest-paid specialties are the three primary care specialties: pediatrics, family medicine, and general internal medicine.
This post is not written to argue that physicians must be paid more. I would submit that if physicians cannot live on $150,000 then we might be doing something wrong...and we are unlikely to get much sympathy from the average person.
Rather, my intent is to note how undervalued primary care services are in our current system of healthcare delivery and payment. Primary care physicians--the physicians who provide comprehensive care, who provide preventive care, who coordinate care--are paid less than all other medical specialists. Radiology and anesthesiology make nearly twice what primary care doctors do; dermatology and anesthesiology make nearly 175% of the average primary care physician.
This is not to say that these medical specialists do not have important roles in providing medical care; however, should a physician who views x-rays and imaging studies be valued at twice the level of the physicians who keep our children well, who monitor their development and intervene if necessary, and who ensure children are fully vaccinated? Should a physician who deals with skin problems be paid at nearly twice the level of a physician who can deal with many of the same skin problems...while also addressing patients' diabetes, blood pressure, heart disease, and mental illness?
The cost of any given service or item depends on its value. Precious metals are expensive because we value them greatly. Luxury cars are expensive because they are highly valued in our culture. Primary care physicians in the US are paid less than all other specialists, and cost less per physician than all other specialists...indicating that the primary care specialties are valued less than other medical specialties.
We have previously noted the importance of primary care to a high-functioning, efficient, and effective healthcare system. Despite the key role primary care should be playing, however, the chart above shows that primary care is not valued at a commensurate level.
Unless we value primary care, and redesign our healthcare delivery and payment systems to reflect this, then we will continue to have a healthcare system that under-performs even as healthcare costs continue to increase. The cost depends on the value: so long as we do not value primary care, then costs will rise even as outcomes do not improve.
This situation is untenable, and must change. We must demand a healthcare system that values those services and specialties that reduce costs. We must enhance primary care's role in our system in order to improve our system's performance. If we change what type of medical care our system values, then we can truly affect cost.
--------------------
Last week, Medscape released the results of their 2011 survey of physician compensation:
I share this post here to point out the discrepancy in physicians' average salaries based on their specialties. In particular, I would like to highlight that the three lowest-paid specialties are the three primary care specialties: pediatrics, family medicine, and general internal medicine.
This post is not written to argue that physicians must be paid more. I would submit that if physicians cannot live on $150,000 then we might be doing something wrong...and we are unlikely to get much sympathy from the average person.
Rather, my intent is to note how undervalued primary care services are in our current system of healthcare delivery and payment. Primary care physicians--the physicians who provide comprehensive care, who provide preventive care, who coordinate care--are paid less than all other medical specialists. Radiology and anesthesiology make nearly twice what primary care doctors do; dermatology and anesthesiology make nearly 175% of the average primary care physician.
This is not to say that these medical specialists do not have important roles in providing medical care; however, should a physician who views x-rays and imaging studies be valued at twice the level of the physicians who keep our children well, who monitor their development and intervene if necessary, and who ensure children are fully vaccinated? Should a physician who deals with skin problems be paid at nearly twice the level of a physician who can deal with many of the same skin problems...while also addressing patients' diabetes, blood pressure, heart disease, and mental illness?
The cost of any given service or item depends on its value. Precious metals are expensive because we value them greatly. Luxury cars are expensive because they are highly valued in our culture. Primary care physicians in the US are paid less than all other specialists, and cost less per physician than all other specialists...indicating that the primary care specialties are valued less than other medical specialties.
We have previously noted the importance of primary care to a high-functioning, efficient, and effective healthcare system. Despite the key role primary care should be playing, however, the chart above shows that primary care is not valued at a commensurate level.
Unless we value primary care, and redesign our healthcare delivery and payment systems to reflect this, then we will continue to have a healthcare system that under-performs even as healthcare costs continue to increase. The cost depends on the value: so long as we do not value primary care, then costs will rise even as outcomes do not improve.
This situation is untenable, and must change. We must demand a healthcare system that values those services and specialties that reduce costs. We must enhance primary care's role in our system in order to improve our system's performance. If we change what type of medical care our system values, then we can truly affect cost.
Tuesday, March 13, 2012
Setting the Stage for the ACA's Second Anniversary
(First published on the National Physicians Alliance blog March 13, 2012)
--------------------
In one week, the Patient Protection and Affordable Care Act (PPACA, or ACA for short) will attain its second anniversary. In preparation for the media attention this milestone will attract, it is necessary to set the stage regarding the ACA's achievements and popularity.
First, a review of what the reforms already in place as a result of the ACA: this timeline provides a good summary, as does this timeline. A review of these timelines shows that the ACA has already led to the following changes:
It can be anticipated that there will be a great deal of critical commentary about how the ACA represents a governmental overreach and that Americans resent this supposed power grab. However, in the most recent Kaiser Family Foundation Health Tracking poll (pdf), 35% of Americans would like to see the law expanded, while 19% would like to see the law kept in its current form. When 54% of the nation would like to leave the law as is or expand its reforms, it is hard to argue that most Americans oppose the ACA in the way that the law's opponents would have us believe: they might highlight that 72% of Americans oppose keeping the ACA in its current form, but 1/2 of that number want the law expanded. This underlines the disingenuous nature of the claims made against the ACA: the law's opponents highlight those bits of data that can be presented as supporting their claims, but conveniently omit the details that undercut their claims.
Opponents of the ACA also have chosen not to propose any replacement for the law any time soon, despite the fact that the House of Representatives actually voted to repeal the law in 2011. While the Republican Party delays action, 1/3 of Americans are struggling to pay their medical bills. This statistic illustrates the reasons that the ACA's reforms were so badly needed: Americans cannot easily afford necessary medical care. The law will address this directly as the health benefits exchanges come online in 2014, but the reforms noted above stand to improve this statistic.
We will certainly hear more and more reasons that the ACA was unconstitutional, especially as the Supreme Court will be hearing arguments on the law's constitutionality the week following the law's anniversary. One of the major arguments against the ACA focuses on the law's mandate that individuals purchase health insurance or face paying a penalty. This article nicely encapsulates arguments as to how and why the ACA and its individual mandate are both constitutional and necessary.
This is where we stand: the ACA is already benefiting Americans, many of whom are in favor of the law's reforms or who would have preferred more expansive reforms. The need for reform is clearly evident, and the ACA's opponents have not proposed any meaningful answer to the current crisis in healthcare access and affordability. Despite the law's opponents' fervent claims and beliefs, the law's constitutionality can be supported in a number of ways.
If you support the ACA's healthcare reforms, get ready, be vocal, and stand tall. The week of March 19-23, 2012 promises to be quite active.
--------------------
In one week, the Patient Protection and Affordable Care Act (PPACA, or ACA for short) will attain its second anniversary. In preparation for the media attention this milestone will attract, it is necessary to set the stage regarding the ACA's achievements and popularity.
First, a review of what the reforms already in place as a result of the ACA: this timeline provides a good summary, as does this timeline. A review of these timelines shows that the ACA has already led to the following changes:
- Young adults can stay on parents' insurance policies until age 26.
- People with preexisting medical conditions who have been uninsured for at least 6 months can access care via Preexisting Condition Insurance Plans.
- Insurance companies can no longer rescind patients insurance, and have eliminated lifetime caps on insurance benefits.
- Children can no longer be denied medical care due to preexisting medical conditions.
- Seniors have received discounts and rebates on their medication costs via Medicare Part D.
- Patients can receive many preventive care services without paying co-pays.
- Funding has been increased for community health centers and for the National Health Service Corps.
- Increased targeting of healthcare fraud.
- Insurance companies will be held accountable for unreasonable premium rate increases, and are being required to spend at least 80-85% of the premiums they receive on providing necessary medical services to beneficiaries.
It can be anticipated that there will be a great deal of critical commentary about how the ACA represents a governmental overreach and that Americans resent this supposed power grab. However, in the most recent Kaiser Family Foundation Health Tracking poll (pdf), 35% of Americans would like to see the law expanded, while 19% would like to see the law kept in its current form. When 54% of the nation would like to leave the law as is or expand its reforms, it is hard to argue that most Americans oppose the ACA in the way that the law's opponents would have us believe: they might highlight that 72% of Americans oppose keeping the ACA in its current form, but 1/2 of that number want the law expanded. This underlines the disingenuous nature of the claims made against the ACA: the law's opponents highlight those bits of data that can be presented as supporting their claims, but conveniently omit the details that undercut their claims.
Opponents of the ACA also have chosen not to propose any replacement for the law any time soon, despite the fact that the House of Representatives actually voted to repeal the law in 2011. While the Republican Party delays action, 1/3 of Americans are struggling to pay their medical bills. This statistic illustrates the reasons that the ACA's reforms were so badly needed: Americans cannot easily afford necessary medical care. The law will address this directly as the health benefits exchanges come online in 2014, but the reforms noted above stand to improve this statistic.
We will certainly hear more and more reasons that the ACA was unconstitutional, especially as the Supreme Court will be hearing arguments on the law's constitutionality the week following the law's anniversary. One of the major arguments against the ACA focuses on the law's mandate that individuals purchase health insurance or face paying a penalty. This article nicely encapsulates arguments as to how and why the ACA and its individual mandate are both constitutional and necessary.
This is where we stand: the ACA is already benefiting Americans, many of whom are in favor of the law's reforms or who would have preferred more expansive reforms. The need for reform is clearly evident, and the ACA's opponents have not proposed any meaningful answer to the current crisis in healthcare access and affordability. Despite the law's opponents' fervent claims and beliefs, the law's constitutionality can be supported in a number of ways.
If you support the ACA's healthcare reforms, get ready, be vocal, and stand tall. The week of March 19-23, 2012 promises to be quite active.
Sunday, March 11, 2012
Poverty in Richmond, Virginia: We Have Our Work Cut Out For Us
Today, I attended the first part of a three part series of presentations focused on the nature of poverty in Richmond, Virginia. Today's presentation was focused on a review of the data; the next will discuss the history that led to this situation, and the final presentation will discuss suggested interventions that might address this issue. The nature of poverty in the city is especially notable because concentrated poverty compounds desperation and leads to hopelessness and alienation. The presentations are based on the work of Dr. John Moeser, of the University of Richmond's Bonner Center for Civic Engagement.
The data is focused on the Richmond Planning District. In 2010, the poverty level for a family of 4 was a yearly income under $22,314. In Richmond City, the rate of those living in poverty increased from 22.1% to 25.8% 2009-2010. Poverty rates rose 18.2%-25.8% 2000-2010. Poverty in the city is at an historical high since 1970. Just as important is the fact that the proportion of those living in poverty in surrounding counties increased from 2000 to 2010 by 94% in Henrico and 71% in Chesterfield. 46% of those in poverty in the Richmond area live in the city; 54% of the region's poor now live in the suburbs. This shift in poverty in the Richmond area reflects a national trend of increasing poverty in suburbs.
There is also a significant level of wealth inequity in the region. In Richmond City, the wealthiest census tract has an average income 17x greater than the poorest. Wealthiest census tract in central VA has an average income 21x the poorest. Despite this great difference between the riches and poorest residents in the city, there is very little physical distance: there are only 3 1/2 miles separating the wealthiest census tract in the city (Windsor Farms) and the poorest (Gilpin Court).
Further details regarding who is poor in Richmond is also striking. Currently, 38% of children in Richmond City live in poverty; this is double the rate from 1990. If one looks at poverty by race, it is notable that 48% of the poor are black. However, the % of all whites and Hispanic community living in poverty have increased. In particular, the % Hispanic community living in poverty increased from 8%-23.5% from 1990-2009. [Editorial note: I think this might represent the fact that the Hispanic community has nearly doubled throughout the Richmond metro area in the last 10 years; many of these newly-arrived individuals and families earn annual incomes below the poverty level.]
Most poor whites live in the suburbs (69%) in suburbs; 61% of all black poor live in the city. Asian and Latino poverty is largely suburban. Overall, Hispanic and black poverty are typically higher density, whether in city or in suburbs; while white poverty less concentrated. More than 20% of the population living in poverty in Richmond City is concentrated in south and east Richmond. 5 census tracts in the city have more than 50% of their residents living in poverty; Gilpin Court has 69% of its residents living in below the poverty line. Concentrated poverty in the City of Richmond is largely found east of Chamberlayne Ave, and on both sides Jefferson Davis Highway south of the river. These areas of concentrated poverty align with the locations of public housing developments. There is no concentrated public housing in counties, but concentrated poverty in the city spills over from the city to the older inner ring of suburbs. There are some census tracts in the city where poverty rates declined, and older housing stock is renovated via gentrification. At the same time, there are some census tracts that have increased in the % of their residents living under the poverty line. Overall, "South Richmond is the city's new East End" with increasingly concentrated poverty. This shift appears to be largely related to increased Hispanic poverty.
For anyone who believes (as I do) that the social determinants of health matter, then this information is striking and relevant. Improving communities' and individuals' health will require more than disease-focused outreach and prevention programs. We will need to refocus on affecting and influencing public policy in such a way as to take health, education, income, etc. into account whenever policy decisions are made. This is less immediate, and perhaps less gratifying, then working one-on-one with patients...but it is equally (or, perhaps, even more) important work. Physicians need to involve ourselves in discussions about policy changes and we need to hold our elected leaders accountable for making decisions that will improve the health status of all people--both by improving healthcare, and by including healthcare considerations when discussion all policy issues.
The data is focused on the Richmond Planning District. In 2010, the poverty level for a family of 4 was a yearly income under $22,314. In Richmond City, the rate of those living in poverty increased from 22.1% to 25.8% 2009-2010. Poverty rates rose 18.2%-25.8% 2000-2010. Poverty in the city is at an historical high since 1970. Just as important is the fact that the proportion of those living in poverty in surrounding counties increased from 2000 to 2010 by 94% in Henrico and 71% in Chesterfield. 46% of those in poverty in the Richmond area live in the city; 54% of the region's poor now live in the suburbs. This shift in poverty in the Richmond area reflects a national trend of increasing poverty in suburbs.
There is also a significant level of wealth inequity in the region. In Richmond City, the wealthiest census tract has an average income 17x greater than the poorest. Wealthiest census tract in central VA has an average income 21x the poorest. Despite this great difference between the riches and poorest residents in the city, there is very little physical distance: there are only 3 1/2 miles separating the wealthiest census tract in the city (Windsor Farms) and the poorest (Gilpin Court).
Further details regarding who is poor in Richmond is also striking. Currently, 38% of children in Richmond City live in poverty; this is double the rate from 1990. If one looks at poverty by race, it is notable that 48% of the poor are black. However, the % of all whites and Hispanic community living in poverty have increased. In particular, the % Hispanic community living in poverty increased from 8%-23.5% from 1990-2009. [Editorial note: I think this might represent the fact that the Hispanic community has nearly doubled throughout the Richmond metro area in the last 10 years; many of these newly-arrived individuals and families earn annual incomes below the poverty level.]
Most poor whites live in the suburbs (69%) in suburbs; 61% of all black poor live in the city. Asian and Latino poverty is largely suburban. Overall, Hispanic and black poverty are typically higher density, whether in city or in suburbs; while white poverty less concentrated. More than 20% of the population living in poverty in Richmond City is concentrated in south and east Richmond. 5 census tracts in the city have more than 50% of their residents living in poverty; Gilpin Court has 69% of its residents living in below the poverty line. Concentrated poverty in the City of Richmond is largely found east of Chamberlayne Ave, and on both sides Jefferson Davis Highway south of the river. These areas of concentrated poverty align with the locations of public housing developments. There is no concentrated public housing in counties, but concentrated poverty in the city spills over from the city to the older inner ring of suburbs. There are some census tracts in the city where poverty rates declined, and older housing stock is renovated via gentrification. At the same time, there are some census tracts that have increased in the % of their residents living under the poverty line. Overall, "South Richmond is the city's new East End" with increasingly concentrated poverty. This shift appears to be largely related to increased Hispanic poverty.
For anyone who believes (as I do) that the social determinants of health matter, then this information is striking and relevant. Improving communities' and individuals' health will require more than disease-focused outreach and prevention programs. We will need to refocus on affecting and influencing public policy in such a way as to take health, education, income, etc. into account whenever policy decisions are made. This is less immediate, and perhaps less gratifying, then working one-on-one with patients...but it is equally (or, perhaps, even more) important work. Physicians need to involve ourselves in discussions about policy changes and we need to hold our elected leaders accountable for making decisions that will improve the health status of all people--both by improving healthcare, and by including healthcare considerations when discussion all policy issues.
#MedRead (part 2) Non-fiction books: Patient narratives, culture, society, and science
This is the second in a series of blog posts that will list books recommended for medical students as a result my asking for suggestions on Facebook and Twitter. This second installment (the first installment can be read here) focuses on society, patient narratives, science, and culture.
In each case, I've linked the book title to its Powells.com listing...mainly because I didn't want to link to larger sites such as Amazon. In practice, I would strongly advise looking for these books at the library (to test them out--use this site to find the books at a library near you) or at your local independent bookstore (such as Chop Suey Books, in Richmond). Remember that if you're local bookseller doesn't carry these titles, they can probably order them for you--and they'll keep your money local.
Alternately, if you wish to support the authors directly, feel free to see if you can purchase the book you are interested in from the author's own website.
The Spirit Catches You and You Fall Down: A Hmong Child, Her American Doctors, and the Collision of Two Cultures – Anne Fadiman
And the Band Played On: Politics, People, and the AIDS Epidemic – Randy Shilts
A Question of Intent: A Great American Battle with a Deadly Industry – David Kessler
Medicine and Human Welfare – Henry Sigerist
Guerrilla Warfare – Ernesto Guevara
28 Stories of AIDS in Africa – Stephanie Nolen
The Year of Magical Thinking – Joan Didion
Autobiography of a Face – Lucy Grealy
Nickle and Dimed – Barbara Ehrenreich
Wretched of the Earth – Frantz Fanon
Pedagogy of the Oppressed – Paulo Friere
Anything by Emily Martin: A good start might be Bipolar Expeditions: Mania and Depression in American Culture
Immortal Life of Henrietta Lacks – Rebecca Skloot
The Match: "Savior Siblings" and one Family's Battle to Heal Their Daughter – Beth Whitehouse
Medial Apartheid: The Dark History of Medical Experimentation on Black Americans from Colonial Times to the Present – Harriet Washington
The Ghost Map: The Story of London’s Most Terrifying Epidemic—and how it Changed Science, Cities, and the Modern World – Steven Johnson
Mountains Beyond Mountains – Tracy Kidder
Treatment Kind and Fair: Letters to a Young Doctor – Perry Klass
As Nature Made Him: The Boy who was Raised as a Girl – John Colapinto
Anything by Richard Feynman: What Do You Care What Other People Think? Further Adventures of Curious Character seems a good start.
A Whole New Life: An Illness and a Healing – Reynolds Price
Mama Might Be Better Off Dead: The Failure of Health Care in Urban America – Laurie Kaye Abraham
Let Us Now Praise Famous Men – James Agee and Walker Evans
Broke, USA: From Pawnshops to Poverty, Inc – How the Working Poor Became Big Business – Gary Rivlin
Barefoot Heart: Stories of a Migrant Child – Elva Treviño Hart
Still Alice – Lisa Genova
Half the Sky: Turning Oppression into Opportunity for Women Worldwide – Nicholas Kristof and Sheryl WuDunn
If you have read these books (or if you recommended them), please use the comments below to provide us with some thoughts on why the book mattered to you.
Sunday, March 4, 2012
#MedRead (part 1) Non-fiction books: Physician Narratives, Medical Practice, and Illnesses
Recently, I made a request on Twitter for suggestions for books that medical students should read. These suggestions could be books of any sort: fiction, non-fiction, clinically-focused, etc. I was hoping to get suggestions for books that made a meaningful impact on people. I'll be posting the lists in a series of blog posts.
In each case, I've linked the book title to its Powells.com listing...mainly because I didn't want to link to larger sites such as Amazon. In practice, I would strongly advise looking for these books at the library (to test them out--use this site to find the books at a library near you) or at your local independent bookstore (such as Chop Suey Books, in Richmond). Remember that if you're local bookseller doesn't carry these titles, they can probably order them for you--and they'll keep your money local.
Alternately, if you wish to support the authors directly, feel free to see if you can purchase the book you are interested in from the author's own website.
The first group includes books that focus on medical practice, physicians' narratives, and the medical aspects of disease:
Every Patient Tells a Story: Medical Mysteries and the Art of Diagnosis – Lisa Sanders
How Doctors Think – Jerome Groopman
The Man Who Mistook his Wife for a Hat – Oliver Sacks
How We Die: Reflections on Life's Final Chapter – Sherwin Nuland
The Case of Doctor Sachs – Martin Winckler
House Calls – Thomas Stern, MD
Anything by Atul Gawande: Complications, Better, and The Checklist Manifesto.
White Coat, Clenched Fist – Fitzhugh Mullan
My Own Country – Abraham Verghese
Of Spirits and Madness – Paul Linde
A Fortunate Man – John Berger
The Coming Plague – Laurie Garrett
Betrayal of Trust – Laurie Garrett
Medicine in Translation: Journeys with my Patients – Danielle Ofri
Not All of Us are Saints: A Doctor’s Journey with the Poor – David Hilfiker
Travels – Michael Crichton
The Motorcycle Diaries – Ernesto Che Guevara
The Great Influenza – John Barry
Final Exam: A Surgeon's Reflection on Mortality – Pauline Chen
The Youngest Science: Notes of a Medicine-Watcher – Lewis Thomas
Aequanimitas – Sir William Osler
White Coat, Black Hat: Adventures on the Dark Side of Medicine – Carl Elliott
The Emperor of All Maladies: A Biography of Cance – Siddhartha Mukherjee
The Demon Under the Microscope: From Battlefield Hospitals to Nazi Labs, One Doctor's Heroic Search for the World's First Miracle Drug – Thomas Hager
Blind Man's Marathon – Steven Hatch
If you have read these books (or if you recommended them), please use the comments below to provide us with some thoughts on why the book mattered to you.
In each case, I've linked the book title to its Powells.com listing...mainly because I didn't want to link to larger sites such as Amazon. In practice, I would strongly advise looking for these books at the library (to test them out--use this site to find the books at a library near you) or at your local independent bookstore (such as Chop Suey Books, in Richmond). Remember that if you're local bookseller doesn't carry these titles, they can probably order them for you--and they'll keep your money local.
Alternately, if you wish to support the authors directly, feel free to see if you can purchase the book you are interested in from the author's own website.
The first group includes books that focus on medical practice, physicians' narratives, and the medical aspects of disease:
Every Patient Tells a Story: Medical Mysteries and the Art of Diagnosis – Lisa Sanders
How Doctors Think – Jerome Groopman
The Man Who Mistook his Wife for a Hat – Oliver Sacks
How We Die: Reflections on Life's Final Chapter – Sherwin Nuland
The Case of Doctor Sachs – Martin Winckler
House Calls – Thomas Stern, MD
Anything by Atul Gawande: Complications, Better, and The Checklist Manifesto.
White Coat, Clenched Fist – Fitzhugh Mullan
My Own Country – Abraham Verghese
Of Spirits and Madness – Paul Linde
A Fortunate Man – John Berger
The Coming Plague – Laurie Garrett
Betrayal of Trust – Laurie Garrett
Medicine in Translation: Journeys with my Patients – Danielle Ofri
Not All of Us are Saints: A Doctor’s Journey with the Poor – David Hilfiker
Travels – Michael Crichton
The Motorcycle Diaries – Ernesto Che Guevara
The Great Influenza – John Barry
Final Exam: A Surgeon's Reflection on Mortality – Pauline Chen
The Youngest Science: Notes of a Medicine-Watcher – Lewis Thomas
Aequanimitas – Sir William Osler
White Coat, Black Hat: Adventures on the Dark Side of Medicine – Carl Elliott
The Emperor of All Maladies: A Biography of Cance – Siddhartha Mukherjee
The Demon Under the Microscope: From Battlefield Hospitals to Nazi Labs, One Doctor's Heroic Search for the World's First Miracle Drug – Thomas Hager
Blind Man's Marathon – Steven Hatch
If you have read these books (or if you recommended them), please use the comments below to provide us with some thoughts on why the book mattered to you.
Sunday, February 26, 2012
Expanding Health Insurance Coverage Should Reduce Costs
(This post was initially published at on the National Physicians Alliance blog, February 26 2012)
--------------------
Without significant changes, healthcare spending in the United States (already one of the highest rates in the world per capita) will continue to increase at an unsustainable rate (PDF). One of the most important goals of the Patient Protection and Affordable Care Act (PPACA) is to control the costs of medical care. Various analyses have discussed the PPACA's potential to reduce healthcare utilization and costs, including this analysis of the law's cost containment features (PDF) and this review of how the PPACA could bend the healthcare cost curve.
However, it can be argued that the key cost savings feature of the PPACA is also the law's defining reform: the PPACA is expected to extend health insurance coverage to nearly 32 million currently uninsured Americans. It can be argued that this expansion of coverage was the underlying crisis that drove the passage of this law, but whether or not expanding healthcare insurance access would reduce costs was unclear.
Now, a new study looks at the impact of extending healthcare access to individuals who previously lacked this access. In November 2000, Virginia Commonwealth University (VCU) Medical Center launched a community-based coordinate care program in response to the health center's role as a principle safety net provider in Richmond, Virginia. Individuals under 200% of the federal poverty level who lacked any other coverage options were eligible for this program. Once enrolled in the program, patients were assigned to a community-based primary care office and these primary care providers received a management fee and fee-for-service reimbursement that were equal to roughly 110% of Virginia's Medicaid fee schedule. This structure would be comparable to enrolling patients in programs that enhance primary care access through either private insurance or public insurance programs such as Medicaid--the two major approaches that the PPACA will take to expanding coverage.
Since this program was implemented, VCU Medical Center has seen a significant change in their system's usage of high-cost services. Primary care visits increased over the period when patients were enrolled in the program, while emergency department visits and inpatient admissions decreased during the same period. This suggests that increased access to primary care services reduces the need for higher-cost emergency department and inpatient interventions. The program also saw inpatient costs fall each year, and total average costs per year per employee fell nearly 50% (from $8,899 to $4,569).
The study's authors conclude that "previously uninsured people may have fewer emergency department visits and lower costs after receiving coverage, but that it may take several years of coverage for substantive health care savings to occur." The authors also noted that there were larger cost savings were achieved in patients with more chronic conditions. This conclusion aligns with prior research including this study, this study, and this article from Dr. Barbara Starfield (PDF).
This new article highlights two important considerations. First: in the program this article describes, increasing individuals' access to health care reduces the overall costs of care. This has significant implications for national healthcare spending trends. Second: as the US population increases its theoretical access to healthcare services, there will need to be primary care physicians available to care for them. The PPACA includes plans to address this workforce need, but other healthcare system reforms (including payment reforms and graduate medical education training) will need to be enacted to meet its full potential.
As the PPACA approaches its second anniversary, and as it moves closer to full implementation in 2014, there is increasing evidence that the reforms embodied in the law will begin bending the cost curve of medical care. This is of critical importance, especially as the political debate in Washington, DC focuses on budgets and deficits. We must support and fully implement the PPACA to help address the nation's fiscal security, as well as providing better and more effective care for our patients.
--------------------
Without significant changes, healthcare spending in the United States (already one of the highest rates in the world per capita) will continue to increase at an unsustainable rate (PDF). One of the most important goals of the Patient Protection and Affordable Care Act (PPACA) is to control the costs of medical care. Various analyses have discussed the PPACA's potential to reduce healthcare utilization and costs, including this analysis of the law's cost containment features (PDF) and this review of how the PPACA could bend the healthcare cost curve.
However, it can be argued that the key cost savings feature of the PPACA is also the law's defining reform: the PPACA is expected to extend health insurance coverage to nearly 32 million currently uninsured Americans. It can be argued that this expansion of coverage was the underlying crisis that drove the passage of this law, but whether or not expanding healthcare insurance access would reduce costs was unclear.
Now, a new study looks at the impact of extending healthcare access to individuals who previously lacked this access. In November 2000, Virginia Commonwealth University (VCU) Medical Center launched a community-based coordinate care program in response to the health center's role as a principle safety net provider in Richmond, Virginia. Individuals under 200% of the federal poverty level who lacked any other coverage options were eligible for this program. Once enrolled in the program, patients were assigned to a community-based primary care office and these primary care providers received a management fee and fee-for-service reimbursement that were equal to roughly 110% of Virginia's Medicaid fee schedule. This structure would be comparable to enrolling patients in programs that enhance primary care access through either private insurance or public insurance programs such as Medicaid--the two major approaches that the PPACA will take to expanding coverage.
Since this program was implemented, VCU Medical Center has seen a significant change in their system's usage of high-cost services. Primary care visits increased over the period when patients were enrolled in the program, while emergency department visits and inpatient admissions decreased during the same period. This suggests that increased access to primary care services reduces the need for higher-cost emergency department and inpatient interventions. The program also saw inpatient costs fall each year, and total average costs per year per employee fell nearly 50% (from $8,899 to $4,569).
The study's authors conclude that "previously uninsured people may have fewer emergency department visits and lower costs after receiving coverage, but that it may take several years of coverage for substantive health care savings to occur." The authors also noted that there were larger cost savings were achieved in patients with more chronic conditions. This conclusion aligns with prior research including this study, this study, and this article from Dr. Barbara Starfield (PDF).
This new article highlights two important considerations. First: in the program this article describes, increasing individuals' access to health care reduces the overall costs of care. This has significant implications for national healthcare spending trends. Second: as the US population increases its theoretical access to healthcare services, there will need to be primary care physicians available to care for them. The PPACA includes plans to address this workforce need, but other healthcare system reforms (including payment reforms and graduate medical education training) will need to be enacted to meet its full potential.
As the PPACA approaches its second anniversary, and as it moves closer to full implementation in 2014, there is increasing evidence that the reforms embodied in the law will begin bending the cost curve of medical care. This is of critical importance, especially as the political debate in Washington, DC focuses on budgets and deficits. We must support and fully implement the PPACA to help address the nation's fiscal security, as well as providing better and more effective care for our patients.
Tuesday, February 14, 2012
Interdisciplinary Service Learning: Una Vida Sana! and Richmond's Hispanic Community
In 2009, I helped start a new interdisciplinary service learning program named "Una Vida Sana!" (A Healthy Life). This program targets cardio-metabolic disease screenings (diabetes, high blood pressure, and high cholesterol) within Richmond's Hispanic Community.
We have now started analyzing some of the data from student participation and our patient data. We reported on the early data analysis at the recent Society of Teachers of Family Medicine (STFM) Conference on Medical Student Education two weeks ago. Below is the presentation from that conference (apologies that the formatting is a little off after the upload):
We have now started analyzing some of the data from student participation and our patient data. We reported on the early data analysis at the recent Society of Teachers of Family Medicine (STFM) Conference on Medical Student Education two weeks ago. Below is the presentation from that conference (apologies that the formatting is a little off after the upload):
Una Vida Sana! STFM Pre-Doc
View more PowerPoint from RichmondDoc
Saturday, February 11, 2012
Where I'm Coming From
(This article originally appeared on Progress Notes on February 9, 2012.)
--------------------
When I entered medical school in Richmond, Virginia, I was certain I wanted to be in primary care but I was not yet sure what specialty. Once I had decided to work in a medically underserved community I chose family medicine because in a rural site, where resources are limited, there is added value in the breadth and scope of family medicine training. I would be able to see all patients, regardless of age, gender, or initial symptoms. This training served me well when I took my first job after residency, in the small town of Keysville, Virginia. In Keysville, I worked for four years providing care to patients in town and in the surrounding counties.
While in Keysville, I helped launch an international medical service and community development in the Dominican Republic in partnership with the College of William and Mary in Williamsburg, Virginia. Working with this project in close partnership with the community of Paraíso, just outside the capital city of Santo Domingo, I have become more aware of the concept of community-oriented primary care. At its heart is the idea that primary care is most effective and most responsive when it is provided in the context of the community. Interventions and care should take into account—and make use of—community resources in order to have the greatest effect. There is little value in a doctor’s recommendation that a patient does not have the resources to follow.
After four years in Keysville, I returned to Richmond to provide care to the Hispanic community and to work more with medical students. Through our department’s International/Inner City/Rural Preceptorship (I2CRP) program, I further developed my understanding of community-oriented primary care and of the importance of social determinants of health – the wide-ranging community and environmental factors that affect health, such as local schools and education, environment and pollution, access to affordable and nutritious foods, and safe public space for exercise. Robust evidence supports social determinants and the need to address them if we wish to improve health (and, perhaps, reduce costs).
Knowing this, I have noticed my perspective changing both on my specialty and on my medical practice. It is increasingly clear that social determinants wield tremendous influence on individual health and that to be effective in primary care we must advocate for change that targets social determinants, but change that is focused on communities’ needs as the community itself identifies them. For example, diet might be difficult to address in a community where the cheapest food is calorie-dense fast food. Exercise might be impractical if patients work late hours and lack safe places to exercise. I believe that we must both keep social determinants in mind as we work with patients and push for reforms that will address (and improve) them.
One-on-one primary care provides notable benefits for the individual, but there is great value in advocating for socially responsible change that will benefit the community at large and, as a result, benefit the individuals we care for. It is not appropriate or sufficient for those outside a community to define what a community’s priorities should be. These priorities should be mutually agreed-upon with the community and should target its key needs.
It is with this combination of motivations and interests that I practice and teach day-to-day. At the heart of all medical care is the one-on-one care provided for the individual patient. This is the core of what we do and what we believe as clinicians, and this relationship and responsibility still carry critical importance. However, we must provide this care with an understanding of the social determinants of health. We must recognize the limits of some of our standard recommendations. Finally, we must begin to connect with our communities. Much of medical education occurs in the sheltered and protected environment of tertiary care centers and classrooms. Students must begin to learn how to look outside of that environment, work with and understand communities, and help build coalitions and partnerships that stand to improve conditions within the communities we serve but to do so on the communities’ own terms.
This is an exciting and challenging time to be in primary care. With our national workforce shortage in primary care, we are both in high demand and heavily worked. For these reasons, we need to train medical students with broad vision, individual focus, and community orientation to provide the medical care that our community and our nation need. I hope to be a part of this solution. It is an important step in making our medical care more efficient and more effective.
Thursday, February 2, 2012
On The Shoulders Of Giants
(This was originally posted on the Occupy Healthcare blog, February 2, 2012)
--------------------
Dr. Barbara Starfield died in 2011. For many people, her name will not stand out. For those of us looking to improve our healthcare system, however, her work is of critical importance.
Dr. Starfield is best known for her work emphasizing the importance and the value of primary care. Primary care (usually focused on family medicine, but including general pediatrics and internal medicine) is the segment of our health care system that focuses on long-term relationships, addressing medical problems from a whole-person perspective, and addressing undifferentiated problems and illnesses. Dr. Starfield wrote in the New England Journal of Medicine that "[i]mportant functions of primary care include serving as the first point of contact for all new health needs and problems; delivering long-term, person-focused care; comprehensively meeting all health needs except those whose rarity renders it impossible for a generalist to maintain competence in them; and coordinating care that must be received elsewhere." This as a concise definition as I have seen for the role of primary care.
In the same article, Dr. Starfield notes that "[r]obust evidence shows that patient care delivered with a primary care orientation is associated with more effective, equitable, and efficient health services. Countries more oriented to primary care have residents in better health at lower costs. Health is better in U.S. regions that have more primary care physicians, whereas several aspects of health are worse in areas with the greatest supply of specialists. People report better health when their regular source of care performs primary care functions well. In addition to features promoting effectiveness and efficiency, there are fewer disparities in health across population subgroups in primary care–oriented health systems"
The article noted above goes on to summarize the evidence that backs up her claim, and I will not post all that evidence here. Similarly, Dr. Starfield authored many, many other articles that provide additional insight on the key roles of primary care in an efficient and effective health care system. I encourage you to review some: if you have taken the time to find this site and read this post, then I presume you have an interest in these ideas. Dr. Starfield's work is a good place to start.
I would like to make myself look smart, and recite all the ways in which our healthcare system fails us on a daily basis. And I would like to pretend that I came up with these ideas on how to fix the system on my own. But, as with so much of life, these ideas are not mine. I try to contribute what I can, but I am building on the work of those who came before--physicians and scholars such as Dr. Starfield. So I would like to present her suggestions (from this interview) as to how we can reform our healthcare system to make it stronger and to improve our nation's health:
--------------------
Dr. Barbara Starfield died in 2011. For many people, her name will not stand out. For those of us looking to improve our healthcare system, however, her work is of critical importance.
Dr. Starfield is best known for her work emphasizing the importance and the value of primary care. Primary care (usually focused on family medicine, but including general pediatrics and internal medicine) is the segment of our health care system that focuses on long-term relationships, addressing medical problems from a whole-person perspective, and addressing undifferentiated problems and illnesses. Dr. Starfield wrote in the New England Journal of Medicine that "[i]mportant functions of primary care include serving as the first point of contact for all new health needs and problems; delivering long-term, person-focused care; comprehensively meeting all health needs except those whose rarity renders it impossible for a generalist to maintain competence in them; and coordinating care that must be received elsewhere." This as a concise definition as I have seen for the role of primary care.
In the same article, Dr. Starfield notes that "[r]obust evidence shows that patient care delivered with a primary care orientation is associated with more effective, equitable, and efficient health services. Countries more oriented to primary care have residents in better health at lower costs. Health is better in U.S. regions that have more primary care physicians, whereas several aspects of health are worse in areas with the greatest supply of specialists. People report better health when their regular source of care performs primary care functions well. In addition to features promoting effectiveness and efficiency, there are fewer disparities in health across population subgroups in primary care–oriented health systems"
The article noted above goes on to summarize the evidence that backs up her claim, and I will not post all that evidence here. Similarly, Dr. Starfield authored many, many other articles that provide additional insight on the key roles of primary care in an efficient and effective health care system. I encourage you to review some: if you have taken the time to find this site and read this post, then I presume you have an interest in these ideas. Dr. Starfield's work is a good place to start.
I would like to make myself look smart, and recite all the ways in which our healthcare system fails us on a daily basis. And I would like to pretend that I came up with these ideas on how to fix the system on my own. But, as with so much of life, these ideas are not mine. I try to contribute what I can, but I am building on the work of those who came before--physicians and scholars such as Dr. Starfield. So I would like to present her suggestions (from this interview) as to how we can reform our healthcare system to make it stronger and to improve our nation's health:
"For health care reform to be successful, the system must focus on providing more primary care to more people. We know exactly what we mean when we say primary care. It is not just having a family physician or internist. It is providing services that achieve four functions. First of all, care has to be accessible, and we know that our care is not very accessible compared to countries that do much better than we do on health.
Second, care has to be person-focused over time. Now, instead of focusing care on meeting peoples' needs, professionals define the needs -- usually in terms of having a specific disease -- and then forget about the people while dealing with the disease. We know from evidence that if you don't deal with people's problems, people are much less likely to get better. We are focusing on diseases that are professionally defined needs. We are not focusing on people-defined needs. Unless we address people-defined needs, we are not going to get good health outcomes.
The third characteristic is comprehensiveness. Instead of referring so much unnecessarily to (sub)specialists, we have to reserve (sub)specialist care for things that (sub)specialists are really needed for -- the less common and complicated things -- and take much better and more care of most health needs within a primary care setting.
The fourth characteristic is coordination. People have to go elsewhere for (sub)specialized services every now and then and that is good care, not bad care. When they do go, the care they receive elsewhere has to be coordinated with their ongoing care.
We know exactly what primary care is, we know exactly why systems organized around it do a better job. It is not a secret, it is not rocket science, but we don't do it."Accessible care, person-focused care, comprehensive care and coordinated care. Simple concepts, and core ideas, that have been lost in our hospital-focused and specialist-heavy system. This is how we change healthcare: identify the beliefs and practices that matter and that work...and then start finding ways to make our system honor and be accountable to them. We don't do it, but we should...and we must.
Subscribe to:
Comments (Atom)
